
Supporting Distributed Teams in Healthcare
Main impacts
- Helped engage wider groups for workplace learning
- Helped turn informal learning into a more structured form of problem solving
The situation before Layers
Highlights
Across the NHS (UK national health service) there are many examples of distributed teams working together on projects to develop and improve systems, services and strategies. These teams often rely on face to face meetings accompanied by emails and sharing of Word documents as a way of keeping their work moving forward. However, this approach can hit problems:
- Discussions and ideas are not always recorded
- Tracking and understanding project development can be difficult where records of discussions are spread across multiple systems
- Wider stakeholder groups (whose buy-in to the projects is essential) often have limited access to or ability to influence the early idea development stage
Description
The NHS is made up of multiple independent organisations (hospitals, General Practices, community care trusts etc) who need to work and learn together, as patient care often involves multiple healthcare professionals and also spans multiple organisations. Separate public bodies exist to support the education/learning/innovation across these NHS organisations. This impact case focuses on the Learning Layers work with distributed teams within two of these bodies (due to the ethical agreements covering this research work we cannot name the bodies):
| Pilot B | Pilot C | |
| Organisation in which team is based | National body | Regional body |
| Team size | 6 members | 5 members |
| Focus of team’s work | Developing strategies and plans for how to effectively use Technology Enhanced Learning (TEL) in healthcare education. | Developing and running quality improvement training and support programmes for the NHS organisations in their region. |
| Team location | Distributed nationally | Distributed regionally |
Team communication and record keeping
Both teams used regular meetings as a key activity to help monitor and move their work forward. For the Pilot C group these were mainly face to face meetings. However, for the Pilot B group there was also occasional use of , Skype or video conferencing for these meetings. In between the face to face meetings the project work tended to be mainly discussed and documented via email and the sharing of Word Documents. The email discussions and face to face meetings did not always involve the whole team.
Team’s engagement of wider stakeholder groups
The way in which the teams currently work is that they (the small team) discuss and develop the ideas (through a mix of email, face to face discussions and document writing) up to a level at which they feel they can share them with the wider group. The ideas are then shared as written documents emailed out to the wider groups for comment or presented and discussed at their infrequent face to face meetings with the wider groups. The wider group in the case of Pilot B could be members of their working groups (approx 20 members in each group) or their total working group membership (approx 100) or much larger numbers when they are communicating across the whole NHS. For Pilot C the wider stakeholder group would have approximately 30-40 members, comprising the trainers in their trainers network.
Team’s key concerns about their current work practice
- The pilot B team’s key concern was that trying to get the work moving forward more quickly.
- The pilot C team wanted to improve their engagement with the wider groups, so that the wider groups would have the opportunity to input into the ideas at an earlier stage.
What Layers did
Highlights
Learning Layers took a participative approach throughout the 4 year project, working closely with healthcare professionals to:
- Identify the pain points in their working/learning practice
- Co-design tools to support their work and informal learning
- Field-test these tools with them from an early stage
- Identify those groups/teams whose work would most benefit from the tools and engage them in the pilots
- Provide face-to-face and online training and support on using the Learning Layers tools
This was undertaken following an iterative, Design Based Research (DBR) approach; in which analyses from empirical studies, learning theories and co-design results are combined to allow us to not only improve the tools but also to reflect on and add to theories and guide the development of the research questions to address in the next design iteration.
Description
Empirical studies In years 1 and 2 of the Learning Layers project we undertook a series of empirical studies in healthcare workplaces. These studies focused on exploring how informal learning took place in the workplace and identifying where technology could provide better support. These studies were run in parallel with and fed into the co-design work.
Co-design and capacity building In each case one or more members of the pilot B and C teams had been involved in the co-design & early field-testing of the Learning Layers tools during years 1 to 3 of the project. During this period, they contributed ideas and feedback into the ongoing development of the tools (Confer & Living Documents in this case), received training on the use of the tools and took part in field-testing of early prototypes.
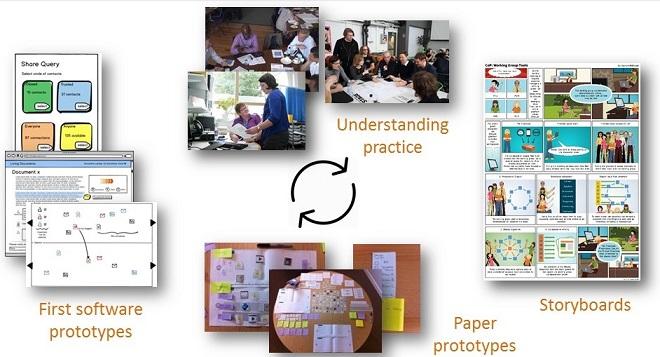
Figure 1: Co-designing with healthcare professionals
Participatory identification of pilot groups and use cases. In year 3 of the project the key healthcare professionals who had been involved in the co-design work were invited to a meeting (Learning Layers Mixing & Matching Meeting) at which all of the Learning tools developed within healthcare were presented both by the Learning Layers healthcare lead, but also by the healthcare professionals who had been involved in their co-design. This meeting gave everyone the chance to see all of the tools and to discuss and consider which tools or combination of tools would best fit the needs of the teams or networks in which they were involved. In discussion with the Learning Layers healthcare team, the healthcare professionals themselves identified the groups who would take part in the pilots and which toolsets they would use.

Figure 2: Two of the tools developed by the Learning Layers project
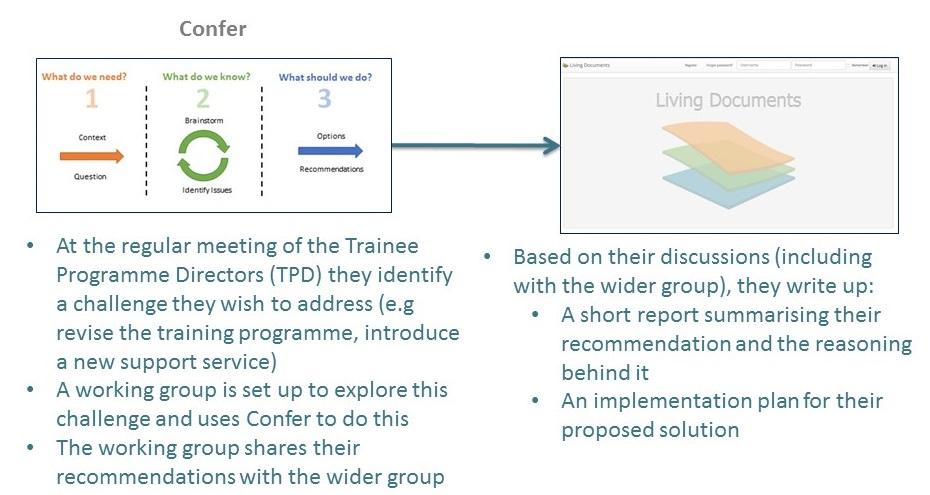
Figure 3: One of the potential use cases discussed at the Mixing & Matching meeting
Tools Pilot. Both teams use of the Learning Layers tools for real work tasks was supported, recorded and analysed over a period of approximately 4 months. In each case the tools (Confer and Living Documents) were introduced to the teams at a 3 hour kick-off workshop (of which about 1.5 hours was training and hands-on use of the tools, the rest was research admin and the evaluation focus group). The team chose a particular problem to explore using the tools during the pilot period. Support (online videos, email support list) and regular contact (weekly hints/tips email to all and regular accompanying conversations with key members of the team) were provided to the teams. An interim workshop (approx 1 hour) was run with each team half-way through the pilot period. At this workshop Learning Layers staff supported the team in using the tools to take their work forward in the meeting itself (e.g. further developing ideas inside Confer) and also collected feedback from the team on their current use of the Learning Layers tools. A final workshop was held during which the participants described their actual use of the tools and the impact it had had.
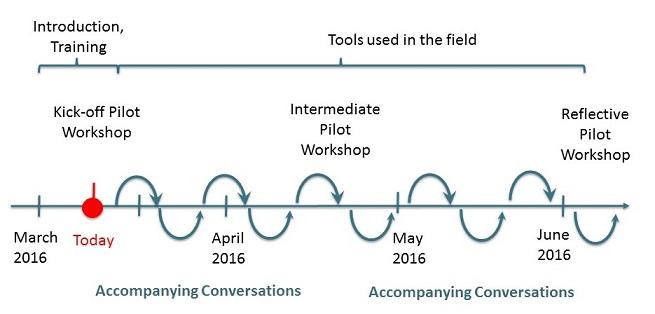
Figure 4: Example timeline showing pilot support activities
Figure 5: An example of a Confer FAQ video. All Confer FAQ videos can be found at http://confer.zone
The situation after Layers
Highlights
A number of positive outcomes and changed practices were observed in both teams:
- The teams reported that the tools supported them in making progress on their real-world tasks.
- The regional team (Pilot C) improved their engagement with their wider groups, as shown by the wider group’s contribution to and shaping of the ideas for a revised training programme.
- The pilot B team commented on how the tools helped them in structuring and recording their discussions during face to face meetings.
- The pilot C team reported on how the progressive inquiry model (embedded within Confer) helped the team to structure and think through their idea development more clearly.
Description
The pilot C team continued to develop their ideas (for a revised training programme) initially through face to face discussions. However, they then used Confer to write up their initial ideas in a way that captured not just the proposal, but also the process by which they had reached this. The 3 step process in Confer (embodying the progressive inquiry model) supported them in doing this. They then used Confer to engage the wider group in the development of these early ideas. They created a Confer web report showing their initial ideas and the process by which they had reached them. They shared this with the wider group and the wider group then sent in comments and additions to the Confer DropZone. Additionally they also used Confer within a face to face meeting with the wider group to review the plans in more detail. The team reported that this worked well and led to the improved engagement with the wider group, who made substantial changes to the initial plans. The wider group also identified ways in which they could use the Learning Layers tools to support their own work and the pilot C team are planning to include Confer as one of the tools that can be used to support quality improvement in their revised training.
It facilitated the discussion so I know it’s for offline discussion but I can see that actually the best use is if when you’re having your meeting you have it on there and type some things in whilst you’re there and then it feels as though you’re adding it on afterwards rather than everybody just go away and do it.
Pilot C participant
one of the guys also had a new novel idea [support for mentoring] for how we could use Confer which he thought it would be very useful in his organisation
Pilot C participant
The pilot B team used Confer within a series of face to face meetings (with the core team) to help with their work on a particular project. They reported that they found it helpful as it structured their discussions and helped them to move the work forward. It also meant that at the end of the meeting they already had their discussion recorded and so no additional minutes needed to be created for this.
…it tends to be very unstructured our discussions and we don’t end up coming to a conclusion and I think it forced us to have that sort of focussed, yeah, that focussed discussion
Pilot B participant
by using Confer it sort of forced us to think about things in a certain pattern, and a certain way of thinking, to come up with solutions
Pilot B participant
Impact that Layers created
Changed learning practices
Our detailed evaluation and analysis of the pilots identified 3 changed practices in pilots B and C. These were how they engaged wider groups in their knowledge building, how they used the tools within face-to-face meetings to capture the discussion and ideas development and how they used the structuring within Confer (progressive inquiry model) to help them to explore the problem space more thoroughly and systematically.
Improved the creation and use of learning resources
The pilot B team were working on the revision of one of their training programmes and wanted to do this in collaboration with their trainers network. The tools allowed them to do this in a way that led to the wider network being able to contribute to and shape the new training programme. The pilot B team believe that this engagement has led to an improved plan for the revised training programme. They also plan to include Confer itself as one of the improvement planning tools that they introduce within their training programme.
Bridging learning contexts
The tools have provided a way for the Pilot C team to get their informal discussions about the problem into a more formal problem-space exploration. They have then also been able to share this problem exploration and proposed solution with a wider group (the trainers who will deliver the training course that is being re-designed) to get their early ideas and feedback. Therefore the knowledge building that would have just happened within the small team has now taken place across the wider group (a network of healthcare organisations).
For Pilot B the tools helped the team to plan how they will communicate their project results to their wider groups. The structured process helped them to identify different key messages that they need to convey to different stakeholder groups.
Links to other sections
- Learning scenarios
- Research methodologies
- Tools
Further Reading
Report of Summative Evaluation in the Healthcare Pilots, [1]
Pilot training and support material
Links to materials used at kick-off workshops (presentation, support material)
Links to support material (videos, example nudge email)
Links to materials used at interim workshop (guidelines)
Contributors
Graham Attwell (PONT), Ed Bellamy (PINBELL), John Bibby (NHS-CCG), Martin Bachl (HSKA), Paul Carder (NHS-CCG), John Cook (UWE), Sebastian Dennerlein, Rose Dewey (NHS-CCG), Raymond Elferink (RAYCOM), Manfred Geiger (UIBK), Paul Hamill (PINBELL), Micky Kerr, Elisabeth Lex, Tobias Ley, Ronald Maier (UIBK), Markus Manhart (UIBK), Patricia Santos (UWE), Christina Sargianni (UIBK), Pjotr Savitski (TLU), Andreas Schmidt (HSKA), Stefan Thalmann (UIBK), Dieter Theiler, Vladimir Tomberg (TLU), Tamsin Treasure-Jones, Lena Waizenegger (UIBK), David Zaki (HSKA)
References
- R. Dewey, M. Geiger, M. Kerr, R. Maier, M. Manhart, P. Santos Rodriguez, C. Sarigianni, and T. Treasure-Jones, “Report of Summative Evaluation in the Healthcare Pilots,” pp. under review, 2016 [Online]. Available at: Link